
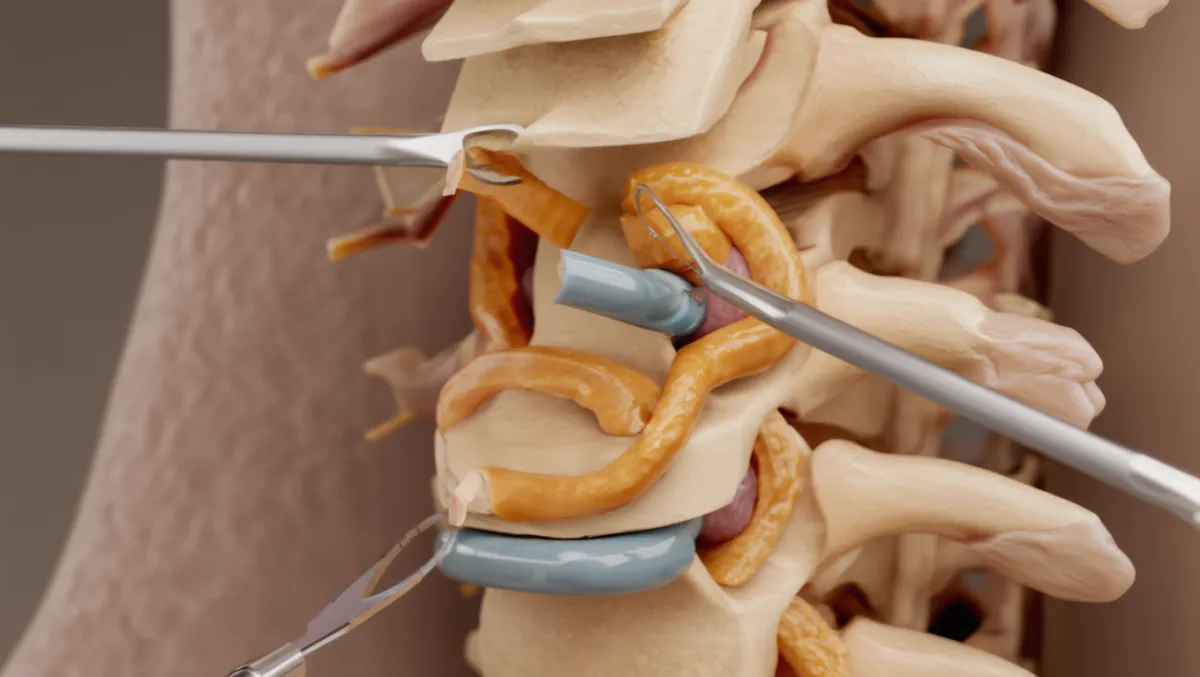
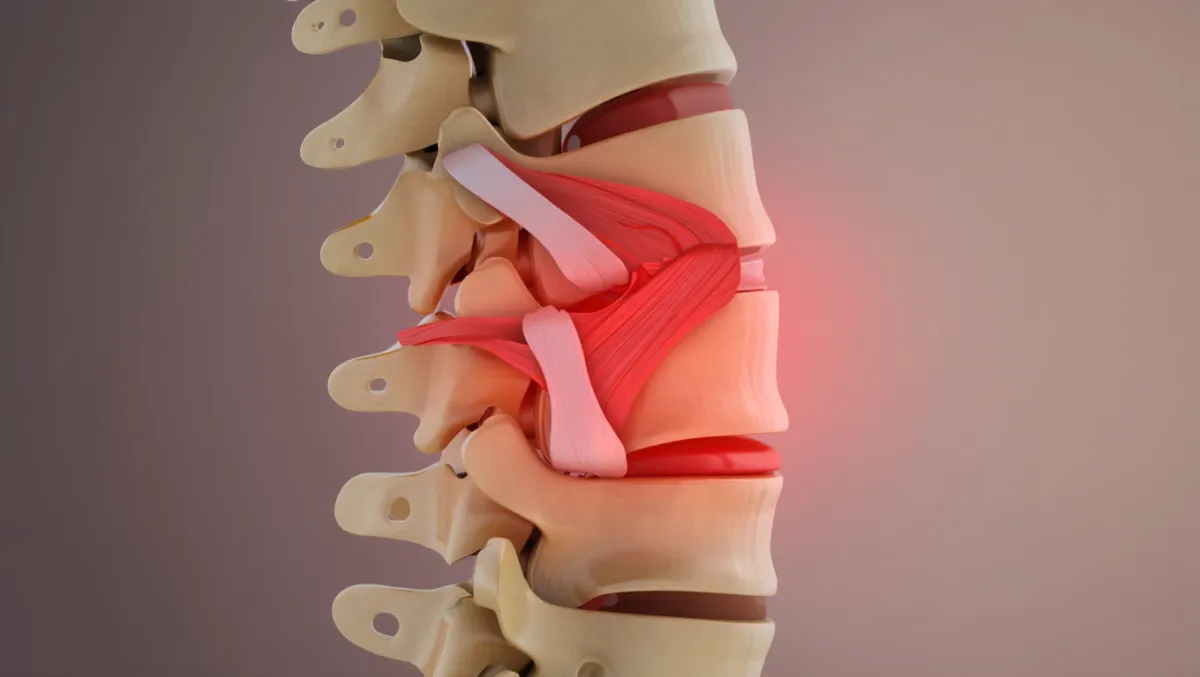
Stenosis
Lumbar Decompression with Coflex Placement
Relieving Stenosis While Preserving Motion
For patients with lumbar spinal stenosis, the classic surgery is decompression (laminectomy or laminotomy). While effective, decompression alone can sometimes leave the spine less stable, leading to fusion. The Coflex® Interlaminar Stabilization® device offers an alternative: after decompression, a small implant is placed between the spinous processes to provide stability without eliminating motion. At Desert Spine and Pain, neurosurgeon Dr. David L. Greenwald, M.D., FAANS, FACS offers Coflex placement for properly selected patients, combining reliable decompression with motion preservation.

Over 100 5-Star Reviews!













Over 30 Years Experience in Orthopedic & Neuro Spine Surgeries.

What Is Coflex?
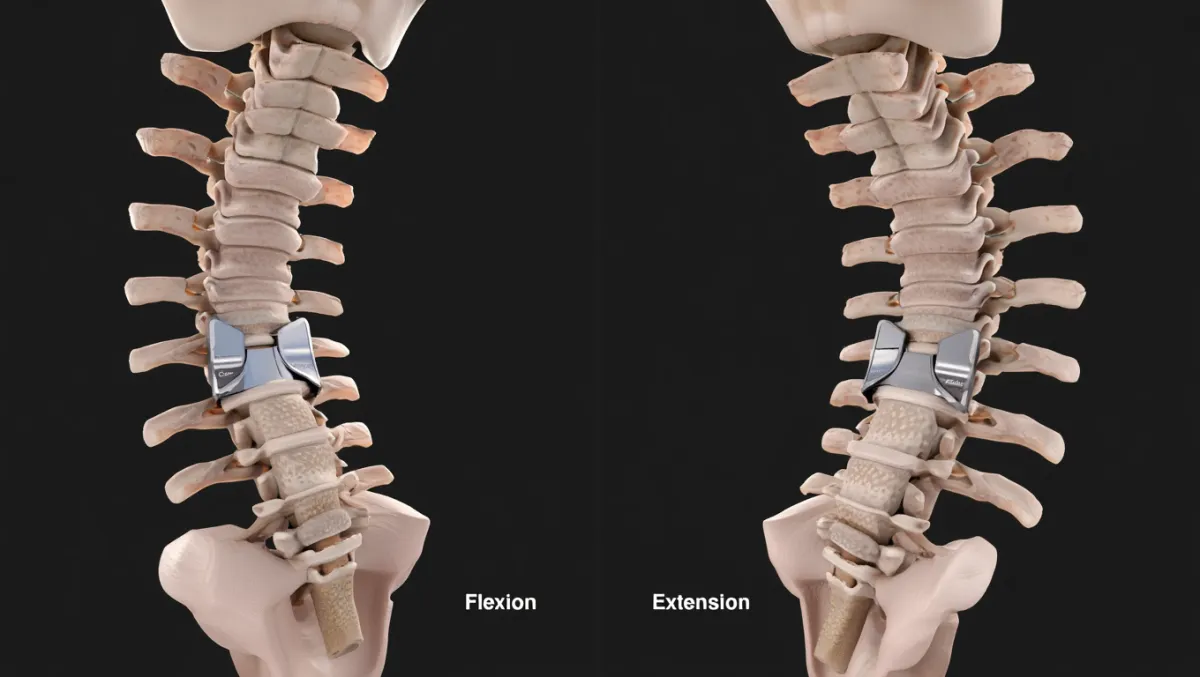
In simple terms: Coflex is a small, titanium U-shaped device placed between the bones in your lower back after decompression. It holds the space open for nerves and stabilizes the spine without fusion.
Scientifically: The Coflex device is an interlaminar dynamic stabilizer implanted after lumbar decompression. It resists extension, maintains foraminal and canal dimensions, and redistributes load, providing stability while preserving sagittal motion at the treated level.
Conditions Treated
Lumbar spinal stenosis causing neurogenic claudication
Back and leg pain relieved by flexion (classic “shopping cart sign”)
Patients who fail conservative care (PT, medications, injections)
Single- or two-level stenosis (typically L1–L5) without instability requiring fusion

Who Is a Candidate?
Good candidates:
Moderate lumbar stenosis confirmed on MRI/CT
No significant spondylolisthesis (>Grade 1)
Desire to avoid spinal fusion if possible
Intact spinous processes
Not candidates if:
Significant instability, deformity, or high-grade spondylolisthesis
Severe osteoporosis or prior laminectomy with spinous process removal
Multi-level disease beyond two levels
The Coflex Procedure: Step by Step
Plain-English Overview
Anesthesia & positioning: You’re asleep under general anesthesia, lying face down.
Lumbar decompression: The lamina and ligamentum flavum are trimmed to relieve nerve pressure.
Implant placement: A small titanium U-shaped device (Coflex) is placed between spinous processes at the treated level.
Stabilization: The device locks in place, supporting the decompressed area while preserving motion.
Closure: The incision is closed; many patients go home the same day or next.
Surgeon-Level Detail
Exposure: Posterior midline or paramedian incision, tubular retractor system possible.
Decompression: Laminotomy/laminectomy ± medial facetectomy to free neural elements.
Sizing: Interspinous space sized using templates; implant chosen accordingly.
Implant insertion: Coflex device impacted between spinous processes; wings expanded to secure position.
Final check: Fluoroscopy verifies placement; device resists extension but allows flexion.
Closure: Layered closure; sterile dressing applied.
Benefits of Coflex Placement
Provides stability without fusion
Preserves motion at the treated level
Faster recovery compared to fusion
Reliable relief of leg pain and neurogenic claudication
Less stress on adjacent levels compared to fusion
Risks & Limitations
Device migration or loosening (rare with correct sizing)
Spinous process fracture (uncommon)
Infection, bleeding, or dural tear (as with any decompression)
Not appropriate for patients with instability, deformity, or osteoporosis
May still require conversion to fusion in the future if degeneration progresses

Recovery Timeline
Day 0–1: Walking the same day; many go home within 24 hours
Weeks 1–2: Light activities, incision care, frequent short walks
Weeks 2–6: Desk work and driving usually resumed
6–12 weeks: Structured physical therapy; progressive return to activity
3–6 months: Strong symptom relief; most activities restored
12 months: X-rays confirm ongoing stability and motion preservation
Why Choose Desert Spine and Pain?
Expert neurosurgeon: Dr. Greenwald is highly experienced in both decompression and motion-preserving procedures like Coflex
Personalized care: Careful patient selection ensures the best outcomes
Minimally invasive focus: Small incisions and precision tools for quicker recovery
Full-spectrum options: From decompression alone to Coflex to fusion, all tailored to your needs
Frequently Asked Questions
How is Coflex different from spinal fusion?
Fusion eliminates motion at the treated level. Coflex preserves motion while providing stability after decompression.
Will Coflex cure my back pain?
It is best for patients whose primary issue is leg pain and walking intolerance from stenosis. Back pain relief is variable.
Can the device move or break?
Device migration is rare when placed correctly. We use meticulous technique and proper sizing to minimize this risk.
How soon can I return to normal activity?
Many patients resume light activities within 2–6 weeks, with full recovery by 3–6 months.
How does Desert Spine and Pain approach Coflex differently?
We emphasize evidence-based patient selection, advanced MIS decompression, and long-term monitoring to maximize safety and effectiveness.



Dr. David L. Greenwald, MD
Neuro-Spine Surgeon

Call Now!
Desert Spine and Pain
A Spine Specialist is standing by.
Relief is just a phone call away!
Available Around the Clock.
Phone: (602) 566-9500
Email: [email protected]

Contact Us

Book a Consultation.
If you’re experiencing lower back or leg pain caused by lumbar spinal stenosis, Lumbar Decompression with Coflex Placement may be the ideal solution to relieve pressure and preserve motion. Dr. Greenwald and his dedicated team will carefully evaluate your condition, review imaging, and determine if you’re a good candidate for this advanced, minimally invasive procedure. Every step you take toward expert spine care brings you closer to comfort, flexibility, and a pain-free life. Schedule your consultation today and learn how Dr. Greenwald’s expertise with Coflex can help you move freely again.

Voted Best Spine Doctor
Over 30 Years Experience in Orthopedic & Neuro Spine Surgeries.
Dr. David L. Greenwald, M.D., F.A.C.S.
Neurosurgeon | Spine Surgeon | Regenerative Medicine
Dr. David L. Greenwald, MD, FACS, is a board-certified spine surgeon with advanced expertise in Lumbar Decompression with Coflex Placement, a motion-preserving alternative to spinal fusion for patients suffering from lumbar spinal stenosis. This minimally invasive procedure involves decompressing the spinal canal to relieve nerve pressure and then implanting the Coflex device, a small titanium spacer that stabilizes the spine while maintaining natural movement. Dr. Greenwald’s precision-guided technique reduces pain, preserves flexibility, and allows for faster recovery compared to traditional fusion surgeries. Patients throughout South Florida trust Dr. Greenwald for his skill in combining innovative technology with compassionate care to help them achieve lasting relief and restored mobility.
Book your Spine Care Consultation Today!

Desert Spine and Pain
Patient Centered & Partner Focused
Quick Links
Resources
Connect With Us
© Desert Spine and Pain. 2026. All Rights Reserved. Sitemap