
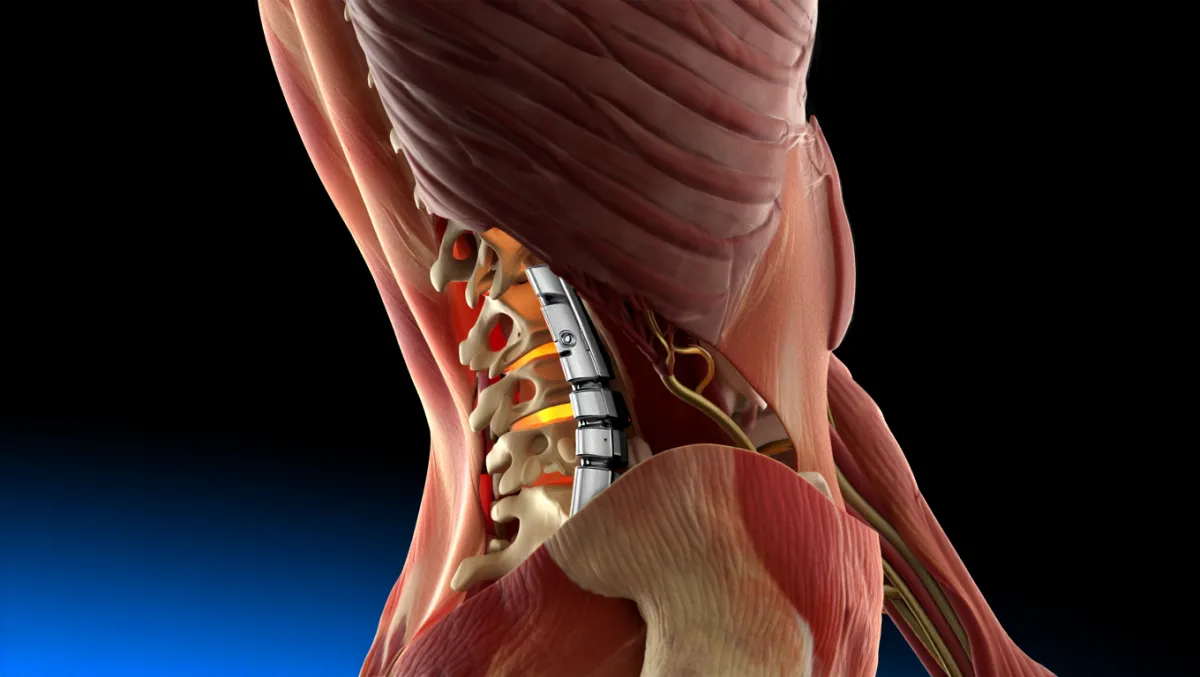
Fusion
Lumbar Fusion
(Anterior, Posterior, PLIF, TLIF, LLIF)
Restoring Stability in the Lower Back
Lumbar fusion is a surgical procedure that permanently connects two or more vertebrae in the lower back. By eliminating painful motion and stabilizing the spine, fusion can relieve nerve compression, correct deformity, and improve quality of life. At Desert Spine and Pain, neurosurgeon Dr. David L. Greenwald, M.D., FAANS, FACS offers a full range of lumbar fusion techniques—including anterior, posterior, and minimally invasive approaches (PLIF, TLIF, LLIF). Each patient’s plan is personalized to their anatomy, symptoms, and long-term goals.

Over 100 5-Star Reviews!













Over 30 Years Experience in Orthopedic & Neuro Spine Surgeries.

What Is Lumbar Fusion?
In simple terms: Lumbar fusion surgery joins bones in the lower back together using bone grafts and implants so they heal into a single, solid structure.
Scientifically: Fusion involves discectomy and/or decortication, placement of an interbody cage or bone graft, and rigid internal fixation (screws/rods/plates). Fusion occurs via osteogenesis, osteoinduction, and osteoconduction over 6–12 months.
Conditions Treated
Spondylolisthesis (slipped vertebra causing instability)
Degenerative disc disease with painful motion
Spinal stenosis requiring decompression and stabilization
Recurrent herniated discs with instability
Trauma or fractures of the lumbar spine
Deformities such as scoliosis (when severe)

Types of Lumbar Fusion Procedures
1. Anterior Lumbar Interbody Fusion (ALIF)
Approach: From the abdomen (anterior)
Advantages: Large cage placement, restoration of disc height and alignment, avoids posterior muscle disruption
Best for: Degenerative disc disease, deformity correction, revision cases
2. Posterior Lumbar Fusion (PLF)
Approach: From the back (posterior midline)
Advantages: Direct decompression of nerves, excellent exposure
Best for: Trauma, deformity, instability after laminectomy
3. Posterior Lumbar Interbody Fusion (PLIF)
Approach: From the back with cages placed into both sides of disc space
Advantages: Direct decompression, strong anterior column support
Best for: Bilateral stenosis, instability needing wide access
4. Transforaminal Lumbar Interbody Fusion (TLIF)
Approach: From the back (posterior paramedian), unilateral corridor
Advantages: Less nerve manipulation than PLIF, MIS options available
Best for: Degenerative spondylolisthesis, recurrent herniations, unilateral pathology
5. Lateral Lumbar Interbody Fusion (LLIF / XLIF)
Approach: From the side (lateral transpsoas)
Advantages: Large cage footprint, indirect decompression, MIS approach with less muscle disruption
Best for: Disc collapse, coronal deformity, foraminal stenosis
The Lumbar Fusion Procedure: Step by Step
Plain-English Overview
Anesthesia: You’re asleep under general anesthesia.
Incision: Front, back, or side depending on approach.
Disc removal: Damaged disc removed; bone surfaces prepared.
Bone graft/cage placement: Cage or graft placed in disc space to maintain height.
Implants: Screws, rods, or plates stabilize the fusion.
Closure: Incision closed; patients walk within hours to days.
Surgeon-Level Detail
Exposure: Anterior retroperitoneal (ALIF), posterior paramedian (TLIF/PLIF), or lateral transpsoas (LLIF).
Discectomy & prep: Annulotomy, nucleus removal, meticulous endplate decortication.
Cage insertion: PEEK/titanium cage sized with lordosis correction; packed with autograft/allograft.
Fixation: Pedicle screws/rods (posterior), anterior plates (ALIF), or lateral plates (LLIF).
Fusion biology: Autograft (iliac crest or local), allograft, BMP, or synthetic bone substitutes.

Benefits of Lumbar Fusion
Provides long-term stability
Relieves nerve compression when combined with decompression
Restores spinal alignment and disc height
Wide variety of approaches tailored to patient needs
Minimally invasive options mean smaller incisions, faster recovery
Risks & Limitations
Infection, bleeding, nerve injury, DVT/PE
Hardware issues or non-union (pseudoarthrosis)
Adjacent segment disease (wear above/below fusion)
Reduced mobility at fused segment
Longer recovery compared to decompression alone
Recovery Timeline
Hospital stay: Outpatient for some MIS cases; 1–3 days for most
Weeks 1–2: Walking encouraged; wound care and light activity
Weeks 2–6: Desk work possible; gradual PT introduction
6–12 weeks: Build activity; restrictions slowly lifted
3–6 months: Most return to normal life; fusion consolidating
6–12 months: Fusion confirmed; clearance for sports and heavy work
Why Choose Desert Spine and Pain?
Comprehensive expertise: Dr. Greenwald performs all major lumbar fusion techniques
MIS focus: Whenever possible, procedures are minimally invasive for faster recovery
Patient-first philosophy: Fusion only recommended when it’s the best option
Trusted outcomes: Proven track record of relieving pain and restoring stability

Frequently Asked Questions
Which lumbar fusion approach is best?
It depends on your anatomy and diagnosis. ALIF restores height/alignment, TLIF and PLIF provide direct decompression, and LLIF offers large cage support with MIS benefits.
Will fusion limit my flexibility?
At the fused level, yes. But most patients notice little difference since other spinal segments compensate.
How long does fusion take to heal?
Typically 6–12 months for solid fusion to form. Smokers or patients with osteoporosis may take longer.
Can minimally invasive fusion work as well as open fusion?
Yes. In the right hands, MIS fusions achieve the same stability with smaller incisions and less pain.
How does Desert Spine and Pain approach lumbar fusion differently?
We offer all approaches—anterior, posterior, lateral—and select the safest, most effective option for your condition.



Dr. David L. Greenwald, MD
Neuro-Spine Surgeon

Call Now!
Desert Spine and Pain
A Spine Specialist is standing by.
Relief is just a phone call away!
Available Around the Clock.
Phone: (602) 566-9500
Email: [email protected]

Contact Us

Book a Consultation.
If you’re living with chronic lower back pain or spinal instability, Lumbar Fusion Surgery may provide the lasting relief and support your spine needs. Dr. Greenwald and his caring team will perform a comprehensive evaluation, review imaging, and discuss which fusion approach—ALIF, PLIF, TLIF, or LLIF—is best for your condition. Every step you take toward expert spine care brings you closer to stability, strength, and an active, pain-free lifestyle. Schedule your consultation today and learn how Dr. Greenwald’s experience in advanced fusion techniques can help you regain confidence and control over your spine health.

Voted Best Spine Doctor
Over 30 Years Experience in Orthopedic & Neuro Spine Surgeries.
Dr. David L. Greenwald, M.D., F.A.C.S.
Neurosurgeon | Spine Surgeon | Regenerative Medicine
Dr. David L. Greenwald, MD, FACS, is a board-certified spine surgeon specializing in Lumbar Fusion Surgery, including anterior (ALIF), posterior (PLIF), transforaminal (TLIF), and lateral (LLIF) approaches. These advanced fusion techniques are used to stabilize the spine, relieve nerve compression, and treat conditions such as degenerative disc disease, spondylolisthesis, spinal instability, or deformity. Dr. Greenwald tailors each procedure to the patient’s unique anatomy and condition, using precision-guided imaging and minimally invasive methods whenever possible. His meticulous surgical approach ensures optimal alignment, pain relief, and long-term spinal stability while promoting faster recovery. Patients throughout South Florida trust Dr. Greenwald for his expertise, compassion, and commitment to restoring their comfort and mobility.
Book your Spine Care Consultation Today!

Desert Spine and Pain
Patient Centered & Partner Focused
Quick Links
Resources
Connect With Us
© Desert Spine and Pain. 2026. All Rights Reserved. Sitemap