
Motion Preservation
Anterior Lumbar Fusion with Disc Replacement
Combining Stability and Motion Preservation in the Lower Back
Some patients with lumbar disc disease need the long-term stability of fusion but still want to maintain motion at certain levels. An advanced option is anterior lumbar fusion with disc replacement, a hybrid surgery that fuses one level while replacing an adjacent disc with an artificial implant. At Desert Spine and Pain, neurosurgeon Dr. David L. Greenwald, M.D., FAANS, FACS performs hybrid fusion/disc replacement procedures for carefully selected patients, restoring stability and relieving nerve compression while maximizing long-term mobility.

Over 100 5-Star Reviews!













Over 30 Years Experience in Orthopedic & Neuro Spine Surgeries.
What Is Anterior Lumbar Fusion with Disc Replacement?
In simple terms: One diseased disc is fused for stability, while another disc is replaced with an artificial disc to keep movement.
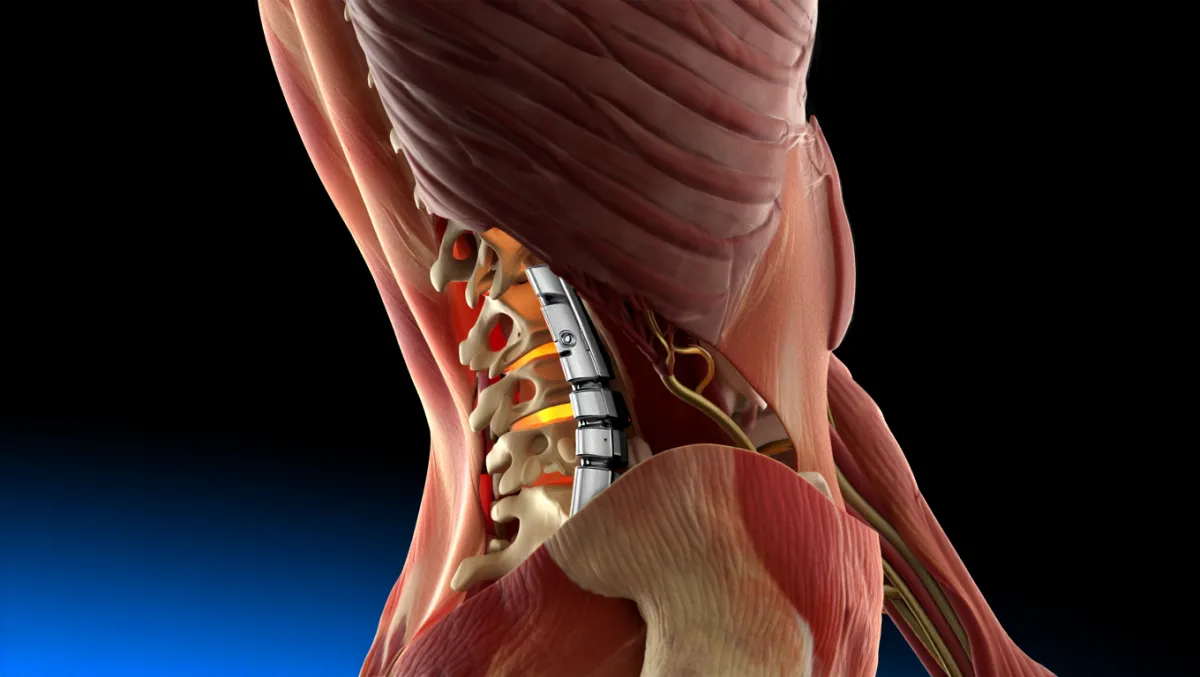
Scientifically: The procedure combines anterior lumbar interbody fusion (ALIF) at one level with lumbar disc arthroplasty at an adjacent level via an anterior retroperitoneal approach, balancing arthrodesis with motion preservation to reduce adjacent segment degeneration.
Conditions Treated
Multi-level degenerative disc disease (1 level requiring fusion, 1 level suitable for disc replacement)
Disc collapse with instability at one level and discogenic pain at another
Radiculopathy or nerve compression from multi-level disc disease
Patients seeking motion preservation while requiring stability
Who Is a Candidate?
Good candidates:
Younger, active patients with 2-level lumbar disease
Healthy bone density, no severe arthritis
Single level unstable (fusion required), adjacent level degenerative but stable (disc replacement possible)
Not candidates if:
Severe multi-level instability
Significant facet arthritis at disc replacement level
Osteoporosis or poor bone quality
Prior fusion at adjacent levels

The Hybrid Procedure: Step by Step
Plain-English Overview
Anesthesia & positioning: You’re asleep under general anesthesia, lying on your back.
Anterior approach: A small incision in the abdomen allows access to lumbar discs.
Disc removal: Diseased discs are removed at affected levels.
Fusion level: One disc space is fused with a cage and bone graft for stability.
Replacement level: An artificial disc is placed at the adjacent level to preserve motion.
Closure: Incision closed; most patients go home in 1–2 days.
Surgeon-Level Detail
Exposure: Anterior retroperitoneal approach with vascular assistance.
ALIF level: Complete discectomy; endplate preparation; interbody cage with autograft/allograft or BMP; anterior plating or integrated fixation as needed.
Disc replacement level: Full discectomy; endplate milling; artificial disc sized and implanted under fluoroscopy.
Final construct: One fused segment plus one mobile arthroplasty segment.
Closure: Layered closure; drains rarely used.
Benefits of Hybrid Fusion with Disc Replacement
Provides stability where needed (fusion)
Preserves motion at adjacent level (disc replacement)
Reduces risk of adjacent segment disease compared to 2-level fusion
Relieves both back and leg pain
Faster recovery compared to multi-level fusion
Risks & Limitations
More complex than single-level surgery
Risks of anterior approach: vascular injury, retrograde ejaculation (men), abdominal organ injury
Implant wear/migration (rare with modern devices)
Fusion non-union possible at fused level
Long-term outcomes depend on careful patient selection

Recovery Timeline
Hospital stay: 1–2 days for most patients
Weeks 1–2: Walking encouraged; light daily activity resumed
Weeks 2–6: Desk work possible; restrictions on lifting/twisting
6–12 weeks: Begin structured physical therapy; strength and flexibility restored
3–6 months: Resume most activities; fusion consolidating, artificial disc functional
6–12 months: Long-term imaging confirms fusion success and disc stability
Why Choose Desert Spine and Pain?
Expert neurosurgeon: Dr. Greenwald specializes in complex hybrid lumbar surgeries
Balanced approach: Fusion where stability is required, disc replacement where mobility matters
Advanced implants: State-of-the-art cages and prostheses with proven durability
Patient-focused care: Surgery only recommended when non-surgical options fail

Frequently Asked Questions
Why combine fusion with disc replacement?
Because some levels require permanent stability, while others can benefit from preserved motion. This balance provides pain relief and flexibility.
Is hybrid surgery better than 2-level fusion?
For the right patient, yes. Preserving motion at one level reduces stress on other discs compared to full fusion.
How long do artificial discs last?
Most are designed for 10–20+ years. Long-term data shows good durability.
How long does recovery take?
Most patients return to normal activities within 3–6 months, with full recovery by 12 months.
How does Desert Spine and Pain perform this differently?
We use neurosurgical precision, MIS techniques, and advanced implants, tailoring surgery to each patient’s anatomy and needs.



Dr. David L. Greenwald, MD
Neuro-Spine Surgeon

Call Now!
Desert Spine and Pain
A Spine Specialist is standing by.
Relief is just a phone call away!
Available Around the Clock.
Phone: (602) 566-9500
Email: [email protected]

Contact Us

Book a Consultation.
If you’re living with chronic back pain caused by disc degeneration or instability, Anterior Lumbar Fusion with Disc Replacement may be the advanced solution you need. Dr. Greenwald and his caring team will thoroughly evaluate your condition, explain your treatment options, and determine whether this hybrid procedure is right for you. Every step you take toward expert spine care brings you closer to comfort, strength, and mobility. Schedule your consultation today and discover how Dr. Greenwald’s surgical expertise can help you achieve long-term relief and restored spinal health.

Voted Best Spine Doctor
Over 30 Years Experience in Orthopedic & Neuro Spine Surgeries.
Dr. David L. Greenwald, M.D., F.A.C.S.
Neurosurgeon | Spine Surgeon | Regenerative Medicine
Dr. David L. Greenwald, MD, FACS, is a board-certified spine surgeon with advanced expertise in Anterior Lumbar Fusion with Disc Replacement, a cutting-edge procedure designed to both stabilize the spine and preserve motion. This technique combines spinal fusion—used to restore stability and alignment—with artificial disc replacement, which maintains natural movement at the treated level. By approaching the spine from the front (anterior), Dr. Greenwald minimizes muscle disruption and reduces recovery time compared to traditional posterior surgeries. This procedure is often recommended for patients with degenerative disc disease, spinal instability, or severe disc collapse. Dr. Greenwald’s precision and patient-focused approach have helped individuals throughout South Florida achieve lasting pain relief, improved function, and a higher quality of life.
Book your Spine Care Consultation Today!

Desert Spine and Pain
Patient Centered & Partner Focused
Quick Links
Resources
Connect With Us
© Desert Spine and Pain. 2026. All Rights Reserved. Sitemap